Joshua Grines, Ella Isaac, Charlie Jespersgaard, Catherine Luong, Hermylie Polanco
This Project explores how medical authority, patient identity, and inequality are constructed through language in Grey’s Anatomy. By analyzing key clinical scenes, we examine how doctors and patients communicate under high-pressure conditions and how power is shaped through speech. Using transcriptions of these interactions, we focus on features such as turn-taking, pauses, and the use of technical medical language. Our findings show that doctors establish authority through extended explanations, directive language, and the use of collective terms like “we,” which present decisions as unified and non-negotiable. In contrast, patients often express themselves through short, emotional questions, reflecting uncertainty and limited control in the interaction. We also find that communication shifts depending on social factors such as race and age, influencing tone, vocabulary, and who is given authority in the conversation. Overall, this analysis highlights how medical dramas reflect and reproduce real-world dynamics of power, expertise, and inequality, showing that authority in clinical settings is not only about knowledge, but also about how language is used.
Keywords: Medical dramas, speech, power dynamics, patients, experts
Introduction & Background
Medical dramas like Grey’s Anatomy make doctors seem powerful, confident, and completely in control, even in chaotic, life-or-death situations. Whether they’re delivering urgent instructions in the ER or explaining a diagnosis to a patient’s family, doctors almost always sound certain, authoritative, and emotionally composed. But have you ever wondered how that authority is actually created? A huge part of it comes down to language, the way doctors speak, the words they choose, and how they structure conversations. In our project, we looked closely at how medical professionals in Grey’s Anatomy use language to establish authority, shape patient identities, and reinforce the hierarchy of the hospital. What we found is that authority isn’t just shown, it’s actively constructed through communication. As a group, we decided to delve further into our question: How do medical TV dramas linguistically construct medical authority, patient identity, and inequality across age, race, and professional hierarchies? We hypothesize that doctors are authoritative through hierarchical speech patterns, using biomedical categorization on patients, and visual staging as experts. In contrast, patients are constructed in subordinate roles through their narratives, often being reduced during moments of institutional decision-making. These dynamics intersect with broader social factors such as age, race, and institutional hierarchy, shaping how patients are addressed and how their experiences are framed.
Methods
We will be making our observations through two different scenes on Grey’s Anatomy, and our method was collecting qualitative data and using basic transcription conventions to analyze.
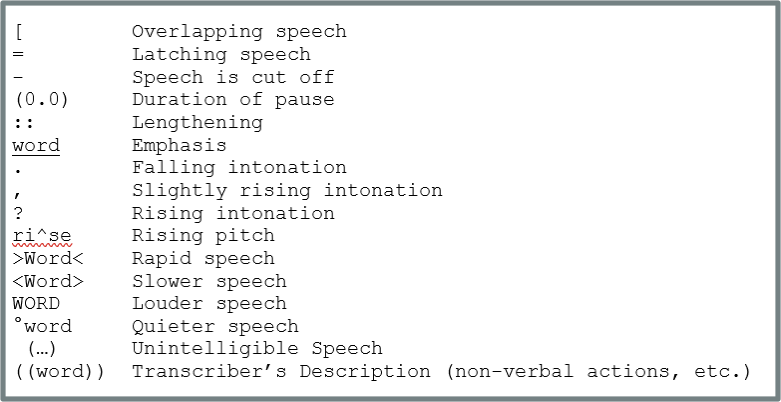
Chart 1: Basic Transcription Conventions
Results & Analysis:

Image 1: In this snapshot from season 2 episode 6 of Grey’s Anatomy, we see a couple (Bonnie and Mr.Maynard) who have been impaled together by a long metal rod surrounded by a medical team. They are being wheeled through a hallway to an emergency room, and what follows is an emotionally heated conversation that displays a negotiation of power and multiple linguistic indicators of medical authority.
Initially, the doctor-patient interaction appears precarious due to the high-stakes nature of the situation and the imbalance of medical authority. The physicians control access to biomedical knowledge, while the patients rely on them to interpret their condition and chances of survival. To reestablish authority in the interaction, the doctors shift the conversation into a biomedical framework through structured explanations and technical speech. This reframes the situation in clinical terms, prioritizing diagnosis and procedural logic over the patients’ emotional experiences.
This dynamic becomes more visible in the following interaction:
- Dr. Shepard: .We have to separate you two.
- Dr. Bruke: <°You would both start bleeding very quickly.>
- Dr. Burke: °Right now, the pole is plugging the wounds.°
- Bonnie: °So (1.35s) if you move me…
- Bonnie: ?I’ll d(^)e?
- ((room is silent))

Image 2: Bonnie’s reaction while Dr. Burke explains to her why the procedure they will use to save Mr.Maynard can not also be used to save her, as it would lead to death.
Through this exchange, biomedical categorization is constructed through technical language such as “bleeding,” “organs,” and “damage,” which abstracts the patients into clinical cases rather than individuals with lived experiences. This reflects a process of recording or entextualization, where patient experiences are transformed into abstract medical categories (Kuipers, 1989). The doctors dominate the interaction through extended turns and uninterrupted explanations, while the patients’ contributions are limited to brief questions. This reflects the institutional organization of medical discourse, where authority is produced through control of knowledge and conversational structure (Ainsworth-Vaughn, 1994).
At the same time, Bonnie and Tom attempt to assert patient narratives through their questions, seeking reassurance and understanding. Tom’s question, “Can’t you just pull the pole out of both of us?” reflects an attempt to negotiate treatment, while Bonnie’s fragmented speech, “So…if you move me…I’ll die?” reveals her effort to process the situation emotionally and cognitively. The use of pauses (0.0), hesitations, and rising intonation highlights uncertainty and vulnerability through paralinguistic features that signal a disruption in conversational flow (Woolfson, 1991).

Image 3: The doctors are surrounding the patients on the table. The rod is still impaling both of them, and the room falls silent as they begin to come to terms with the fact that the procedure may lead to Bonnie’s death.
Notably, silence plays a critical role in this interaction. After Bonnie realizes her likely death, the room becomes silent, marking a breakdown in ordinary conversational flow. This pause signals the limits of biomedical discourse, as the technical explanation gives way to an unspoken acknowledgement of morality. In this moment, the patient narrative briefly resurfaces, but it is not fully engaged or responded to, reinforcing how institutional priorities override individual experience in high-pressure medical settings. This interaction demonstrates how medical authority is not only conveyed through what is said, but through how it is said; through pacing, control of turns, and the strategic use of silence.

Image 4: We see the family of the 12-year-old boy who was shot facing the cop who believed him to be a burglar. They are standing in a hospital hallway with the patient lying on a stretcher, all while the doctors observe from a few paces back.
At first glance, Grey’s Anatomy’s interactions appear to follow a standard medical hierarchy in which physicians exercise authority through diagnosis and decision‑making. Yet the scene demonstrates that healthcare power extends beyond clinical expertise. Authority is shared among doctors, police, and family members, each representing different institutional, emotional, or experiential forms of power (Ainsworth‑Vaughn, 1994).
This layered dynamic becomes clear in the following exchange:
- Father: I wa:nt to thank you kindly to <step away> from my twelve-year-old _child_.
- Mother: He always forgets his keys. >Were you climbing in the wi:ndow again?<
- Patient: Ye:s, but I di:d go to the nei:ghbor’s house fi:rst,
- Mother: And for <thi:s> you sho:t hi:m?
- Patient: I was re:aching for my phone to call you, (0.2) and they sho^t me
- Officer: Why don’t you c:al:m down.
- Mother: Ca:lm down? Calm do^wn?
- Officer: Calm down. We will have a lit:tle discussion about it.
- Doctor: [You mean after they have had some ti:me with their kid (0.2) right?
In the case of Eric Sterling, a young Black child shot by a police officer, clinical authority lies with the physicians directing care, while the officer embodies institutional power tied to the incident’s cause. The parents, meanwhile, attempt to assert emotional and moral authority on behalf of their child. These layers of authority are not equal; institutionally supported voices tend to dominate, illustrating how medical encounters reproduce broader social hierarchies (Wilce, 1997).
The parents’ attempts to assert themselves (“step away from my child”; “And for this you shot him?”) are ignored, while the officer’s directives aim to silence alternative accounts. The child’s own explanation, “I was reaching for my phone…”, is overshadowed by institutional voices. This dynamic mirrors real healthcare settings, where families not only face medical hierarchies but also racialized power structures that influence whose narratives are taken seriously. Research shows that physicians interrupt minority patients more frequently, reinforcing control over the interaction (Kuipers, 1989).
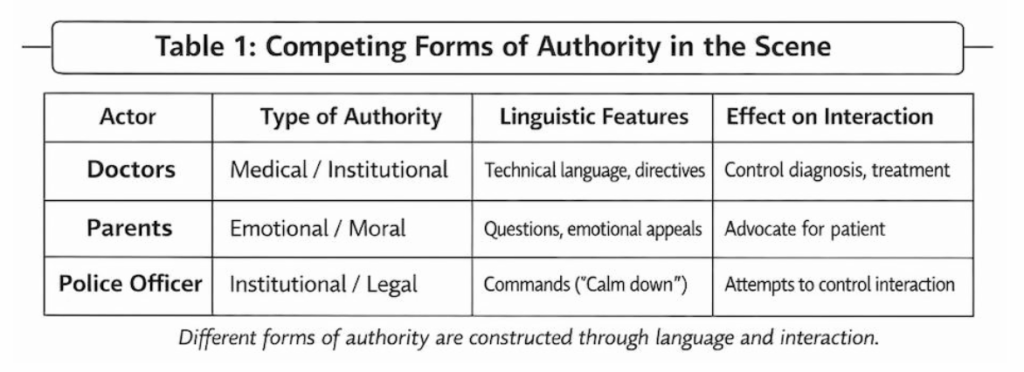
Table 1: This table aims to show what type of authority and linguistic features each character in the scene possesses and how they influence the interaction we have analyzed.
The scene also illustrates how patient and family voices can be minimized through the use of medical and institutional language. While doctors focus on diagnosis and treatment, the police officer attempts to control the interaction through directives such as “calm down,” the emotional and experiential perspectives of the family risk being overshadowed. In this context, the child’s injury is reframed primarily as a clinical problem, reflecting a process of entextualization in which lived experience is detached from its social context and translated into biomedical categories (Kuipers, 1989).

Image 6: After the police officer attempts to tell the mother to “calm down”, we see her clearly upset and snaps back at the ignorant remark made by the cop while her son is lying on a hospital bed next to her.
While this reframing is necessary for treatment, it also shifts attention away from the broader social context of the injury, including the role of racial profiling and police violence. The family’s emotional and experiential perspectives are not validated; instead, they are managed, minimized, or redirected. The doctor later challenged the officer, “after they have had some time with their kid, right?”, momentarily disrupting police authority, but does not fundamentally alter the institutional hierarchy. By redirecting and containing these responses, the interaction disempowers the family, effectively rendering their narrative secondary within the clinical encounter (Wilce, 1997).

Image 7: The patients Mom, Dad, and two siblings stand in the room where the patient is being treated, all looking at him with concern. His brother, in particular, is clearly appalled by the situation.
By depicting these dynamics, Grey’s Anatomy highlights how communication in medical settings can both address and inadvertently suppress elements of patient experience. The scene presents that who is heard, and how their words are interpreted, is shaped not only by medical necessity, but also by underlying social inequalities.
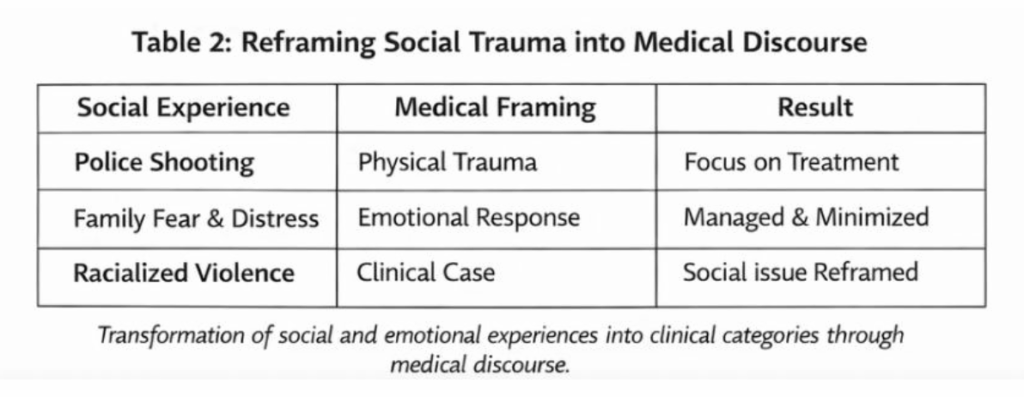
Table 2: This table aims to show how each unique social experience shown in the episodes is viewed through the lens of medical professionals and then treated.
Discussion & Conclusions:
This pattern supports our initial hypothesis that medical dramas portray doctors as authoritative from both linguistic control and professional hierarchy. Across the scenes, we found that authority is constructed through directives, technical language, and conversational control. These patterns reveal how doctors must process situations logically to make decisions that are realistic in life-or-death situations. Patient experiences are often reframed as biomedical categories, and communication patterns shift depending on social factors such as age and race. These linguistic and interactional patterns reflect a larger cultural phenomenon in which media normalize institutional hierarchies and shape expectations about how real clinical encounters should sound. Their narrative isn’t diminished in these settings; rather, they are given the “reality” of things. Our findings should be interpreted with several limitations, as our analysis focuses on a small set of scenes from a single television show. Nevertheless, these scenes still provide insight into how popular media represent medical authority and patient identity and how certain voices are positioned as more legitimate within that representation.
References
Ainsworth-Vaughn, N. (1998). Is that a rhetorical question? Claiming Power in Doctor–Patient Talk, 103–124. https://doi.org/10.1093/oso/9780195096064.003.0006
Burson‐Tolpin, A. (1989). W. H. R. Rivers prize essay (1988): Fracturing the language of biomedicine: The speech play of U.S. physicians. Medical Anthropology Quarterly, 3(3), 283–293. https://doi.org/10.1525/maq.1989.3.3.02a00070
Kuipers, J. C. (1989). “medical discourse” in anthropological context: Views of language and power. Medical Anthropology Quarterly, 3(2), 99–123. https://doi.org/10.1525/maq.1989.3.2.02a00010
Wilce, J. M. (1997). Discourse, power, and the diagnosis of weakness: Encountering practitioners in Bangladesh. Medical Anthropology Quarterly, 11(3), 352–374. https://doi.org/10.1525/maq.1997.11.3.352
Woolfson, P. (1991). Aspects of non‐verbal accommodation to language in a bilingual Montreal Hospital setting. Journal of Linguistic Anthropology, 1(2), 178–188. https://doi.org/10.1525/jlin.1991.1.2.178